Ligament Injuries and ACL Reconstruction
The ACL and Ligaments of the Knee
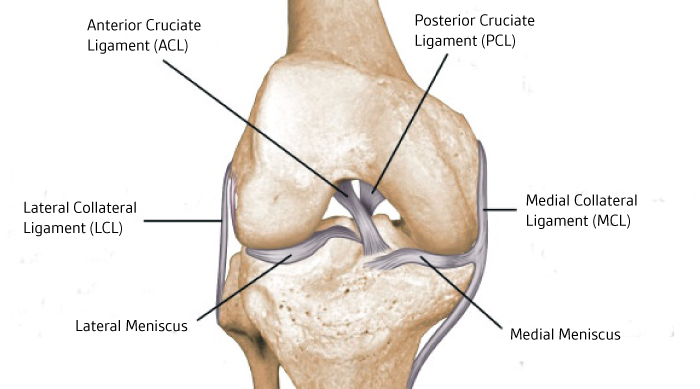
There are four main supporting ligaments of the knee, the Anterior Cruciate Ligament (ACL), the Posterior Cruciate Ligament (PCL), the Medial Collateral Ligament (MCL), and Lateral Collateral Ligament (LCL). These connect the tibia and femur, and both stabilise and guide the knee during motion. These ligaments can be injured during sporting activity or in other accidents, leading to pain, swelling, limp, and potentially a loss of stability. Depending on the ligament injured, and the severity of the injury, and whether the knee is unstable, the ligament may need to either be braced while it heals, surgically repaired, or surgically reconstructed.
Medial Collateral Ligament (MCL) Injuries
Most of these injuries do not require surgery, but may need a period of bracing. A hinged knee brace is used to support the knee and unload the MCL while it heals. Typically this takes 6-12 weeks. Very unstable injuries, which are usually associated with other ligament or meniscus tears, may require repair or reconstruction.
Lateral Collateral Ligament (LCL) Injuries
These injuries are usually sustained in high-energy accidents, and usually require reconstructive surgery and a period of bracing. They may also be frequently associated with injuries to other ligaments or the common peroneal nerve, which helps to lift the foot.
Posterior Cruciate Ligament (PCL) Injuries
These are more rare than ACL injuries, and are often from hyperextension of the knee. Low grade injuries often settle well with bracing, but severe (grade 3) injuries may require surgical reconstruction.
Anterior Cruciate Ligament (ACL) Injuries
ACL injuries are very common, and frequently require surgical management. The next section covers the ACL in detail.
Anterior Cruciate Ligament (ACL) Reconstruction
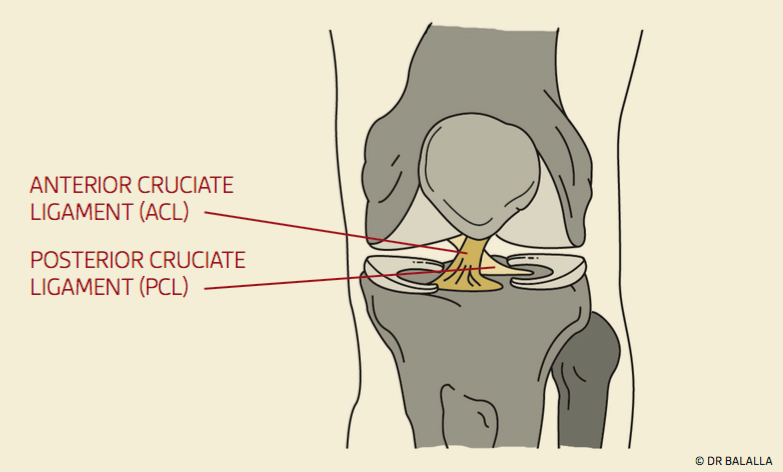
The anterior cruciate ligament, or ACL is one of the major stabilizing ligaments of the knee. It is a strong, thick structure that runs from the femur (thigh bone) to the tibia (shin bone) and lies in the centre of the knee joint.
It has a major role in guiding the knee during movement and prevents abnormal rotation and front-to-back movement of the femur on the tibia. Absence of a functioning ACL due to injury may manifest itself as the knee giving way, particularly during twisting movements.
The ACL is most commonly injured during sporting activity. Most injuries are sustained while the injured leg is planted on the ground and the athlete is performing a movement that twists their knee, such as changing directions while running. Most injuries do not involve a collision with another player.
At the time of an ACL injury, patients experience sudden, severe pain. There is often a sensation of the knee falling inwards in a “knock-kneed” way. An audible ‘pop’ may be heard, and the athlete usually falls to the ground and cannot resume play. The knee usually swells immediately, and may remain swollen for several weeks. Crutches are often necessary for a week or two following injury.
The pain, inflammation, and persistent fluid within the knee can make bending the knee difficult for several weeks.
There can be a persistent pain over the inner aspect of the knee due to an injury to the medial collateral ligament (MCL) which is often injured in association with an ACL injury. A knee which locks and cannot fully straighten may indicate a concurrent injury to the meniscus, which has become entrapped and is preventing the knee from extending.
It is important to differentiate an ACL injury from other injuries that have a similar mechanism and pattern of symptoms – for example, a patella dislocation, or an isolated meniscal tear.
Patients without an ACL may experience instability of their knee. This manifests itself as the knee “giving way”, particularly during twisting or pivoting activity. Prolonged instability may lead to an injury of the meniscus. Meniscus tears can cause locking, clicking, catching, and sharp joint-line pain.
If the meniscus is injured, and loses its ability to share load and absorb the forces of weight bearing, this may lead to premature arthritis of the knee.
An ACL injury can be diagnosed by careful physical examination. However, this can be difficult in the recently injured knee due to swelling, pain, and restriction of motion. In a very swollen, painful knee, other diagnoses such as patella dislocation and multi-ligament injury must also be considered.
Plain x-rays do not image the ACL, and usually only show the presence of fluid or blood within an injured knee joint. Occasionally, plain X-rays may show a small fracture at the edge of the outer tibia, called a Segond fracture.
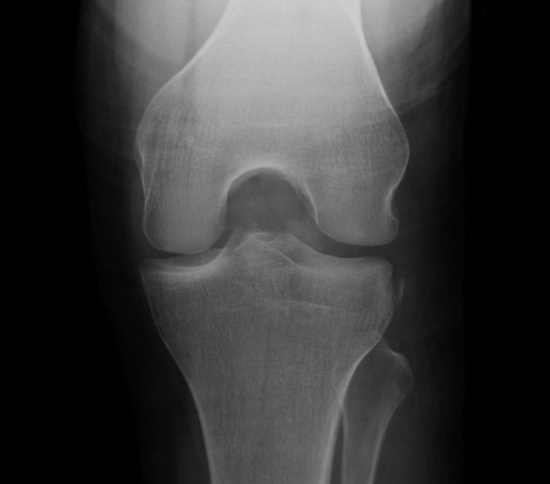
The Second fracture is visible at the lateral edge of the tibia. Although the ACL is not attached directly, this fragment can be pulled off the bone as the ACL ruptures.
In rare cases, more commonly in teenagers and young adults, the ACL will tear from the tibia with a bony fragment. This is known as a tibial spine avulsion fracture. These avulsions behave differently, and can be repaired surgically, rather than needing reconstruction.
Ultrasound is not able to adequately visualise a tear of the ACL.
The most useful imaging test is the MRI scan. This is similar to a CT scan, but involves no radiation, instead using a strong magnetic field. It provides excellent soft tissue imaging of the entire knee, and is able to provide information on not only the ACL, but the condition of the menisci, and the other ligaments of the knee. If the meniscus is also injured, this is best addressed at the time of the ACL reconstruction.
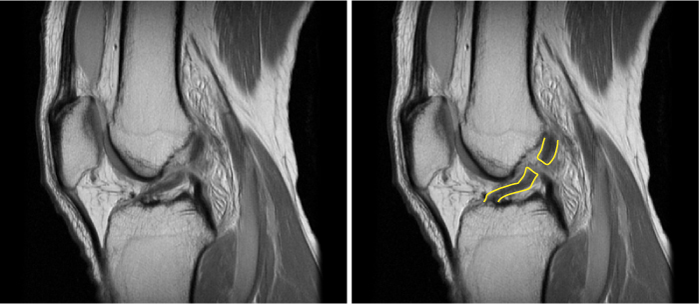
MRI of a ruptured ACL. In an uninjured ligament, the fibres run very straight, with no interruption.
Instability of the knee can cause injury to the meniscus, or to the articular cartilage. Repeated episodes of giving way can tear the meniscus, which acts as a shock absorber on each side of the knee. The loss of a meniscus can be devastating in a young patient, as the increased loads and stresses borne by the articular cartilage can lead to premature arthritis.
It is well recognised that loss of the ACL increases the risk of damage to the meniscus. It is also known that absence of a meniscus increases the risk of arthritis. Many surgeons advocate reconstruction of the ACL in younger patients to prevent arthritis later in life secondary to meniscal injury.
The decision to reconstruct the ACL depends on three factors:
Age
Younger patients are thought to benefit from the meniscal protective effects of reconstruction, and tend to have higher functional requirements.
Symptomatic Instability
Patients who have a knee that gives way during activity will require a reconstruction, where those without noticeable instability may be able to function well without surgery.
Functional Demands
Patients who are content to limit their activity, and avoid activities which involve pivoting or sudden changes of direction, can function well without surgery, but those wishing to do more demanding activity may benefit from reconstruction.
Repair involves keeping the original tissue, and approximating the ends which then go on to heal. Attempts at repair of ACL tears have been largely unsuccessful.
Reconstruction involves replacing the damaged tissue with a substitute tissue called a graft. This tissue is most frequently from the same patient, but can be from another donor, or a synthetic material. Reconstruction can be anatomical or non-anatomical. Anatomical reconstruction involves placing the graft in the usual location for the damaged structure. This is the most frequently performed type of reconstruction. Non-anatomical reconstructions place the graft away from the usual position of the damaged structure, but are designed to mimic its effect. This is most commonly performed in reconstruction in children, where anatomic reconstruction may injure the growth plates.
This depends on your age, symptoms, and expectations of future activity. This is best discussed following a thorough history and physical examination.
Reconstruction is best performed on a knee with minimal swelling which is bending well. In general, you can choose the timing of your reconstruction to suit your circumstances at work or home. However, if the knee is locked due to a meniscal tear, or is grossly unstable and giving way frequently, more urgent treatment may be required.
Most techniques involve initially obtaining and preparing graft material. These are discussed below. The knee is then assessed arthroscopically, and any tears of the meniscus repaired. The insertion sites of the ACL on the femur and tibia are identified, and tunnels drilled from those insertion sites through the tibia and femur respectively.
The graft is then passed though the tunnels, with some of the graft material sitting within the joint. This part inside the joint forms the new ligament. The graft can be fixed at each end by a variety of devices. My preferred technique is discussed further on.
There are many potential graft choices in ACL reconstruction. Each has its pros and cons.
Hamstring tendons
Two tendons from the inner aspect of the knee are detached and folded to make a four-strand graft. This is a very strong graft, and has excellent long-term results. It can be taken via a small incision on the inner aspect of the knee. It is well tolerated and in most cases hamstring function is not impaired.
Patella tendon with bone blocks
This graft is perhaps a little stiffer than a hamstring graft, and is also commonly used. The graft is the middle third of the patella tendon, which runs on the front of the knee from the kneecap to the shinbone. It requires a bigger incision than for a hamstring harvest, and has been associated with pain on kneeling. It is an excellent option for a revision (re-do) reconstruction.
Allograft
This is sterilised graft material from a cadaveric donor, and as such there are no harvest-site problems for the patient. Australian regulations mean that only irradiated graft is available. Irradiated graft is inferior to fresh tissue, as it is weaker and takes longer to incorporate. There are also concerns with potential infection.
Quadriceps tendon
This involves taking a segment of the tendon above the kneecap, with or without part of the kneecap bone. This graft is quite well tolerated, but requires a less cosmetically appealing incision on the front of the knee.
Synthetic ligaments
Synthetic ligaments are appealing due to the lack of any problems with the harvest of tissue. However, historically they have had a high failure rate, often due to an inflammatory reaction within the knee. The most recent synthetic ligament, the LARS, has not shown such a high rate of complications, but concerns still persist. The LARS relies on preservation of the ruptured ligament stump, and acts as a splint for healing.
The native ACL contains nerve fibres and blood vessels, as well as the collagen fibres which constitute the ligament. In most ACL reconstructions, this remnant is removed to allow easy access to the intercondylar notch of the femur. In the remnant preservation technique, which I use, the entire ACL remnant is left in place, and the graft shuttled through this. Studies have show that remnant preservation improves revascularisation time, graft strength, and sense of joint position.
My preferred technique for ACL reconstruction is to use a single hamstring tendon from the same leg as the reconstruction. The tunnels are created using arthroscopy (keyhole surgery). These tunnels are positioned precisely using a modern “anatomical” technique. I preserve the patients original ACL stump, and route the graft though it. The original ACL surrounds the graft like a sleeve. I feel that this technique provides more healing tissue, as well as blood supply and nutrition, and perhaps also preserves the nerves which were within the original ACL, leading to improved sensation of joint position. The graft is fixed to the femur using a loop and button device, and to the tibia via another adjustable loop and button. Local anaesthetic is widely infiltrated around the knee, and there is no post-operative brace. Patients walk out of hospital on crutches on the same day or the day following surgery.
Watch a video of the surgical technique below. Note that this video does not show the original ACL remnant being preserved.
Walking
Patients walk out of the hospital on the day of surgery, or the day after surgery, and are encouraged to put their full weight through the operated leg. Crutches are usually needed, but for no longer than two weeks after surgery. Most patients discard their crutches after less than a week.
Driving
Driving is permitted when legs operating pedals are pain free, bending comfortably, and pain medications have ceased.
Heavy lifting
This is permitted after 6 weeks. Deep squats are allowed, as long as there is no twisting. If a meniscal repair has also been performed, loaded squats are permitted after 3 months.
Running
Straight line running can commence after 6 weeks.
Cutting/Pivoting activities
These can commence after 3 months, but under physiotherapist supervision. Sport-specific drills at 6 months.
Contact sport
9 months after reconstruction.
That is the aim of reconstruction. However, the individual outcome depends on the presence of other damage within the joint, successful incorporation of the graft, and satisfactory rehabilitation.
There are general risks associated with knee arthroscopy, as well as specific risks for graft harvest and reconstruction.
General risks of surgery
These include adverse reaction to medications, pain, bleeding, infection, stiffness, blood clots in the calf (deep venous thrombosis or DVT), blood clots traveling from the calf to the lungs (pulmonary embolus).
Risks specfic to hamstring graft harvest
- Many patients experience discomfort on the inner thigh, which feels much like a hamstring sprain. This sensation typically lasts a few weeks.
- Retraction of the saphenous nerve which runs near the tendons may cause altered sensation over the inner calf and foot area. This usually resolves completely.
- Most patients are left with a small area on the outside of the graft harvest incision where sensation is diminished. This is usually permanent but well tolerated, with no associated weakness of the muscles
- Some patients have reduced hamstring power even years after harvest. With two hamstrings tendons harvested this can be up to 20%, but is less with a single hamstring technique.
Risks specific to ACL reconstruction
- Stiffness after surgery may take several months to resolve.
- Synovitis, which is swelling of the knee, may peak at around 2 months, but usually resolves at around 3 months.
- The graft may stretch out with time, leading to a recurrence of instability.
- The graft may rupture on return to sporting activity, in much the same way as the original injury.
- There is an increased risk of arthritis following ACL rupture. This risk is increased in some way even despite reconstruction.
The anterior cruciate ligament (ACL)
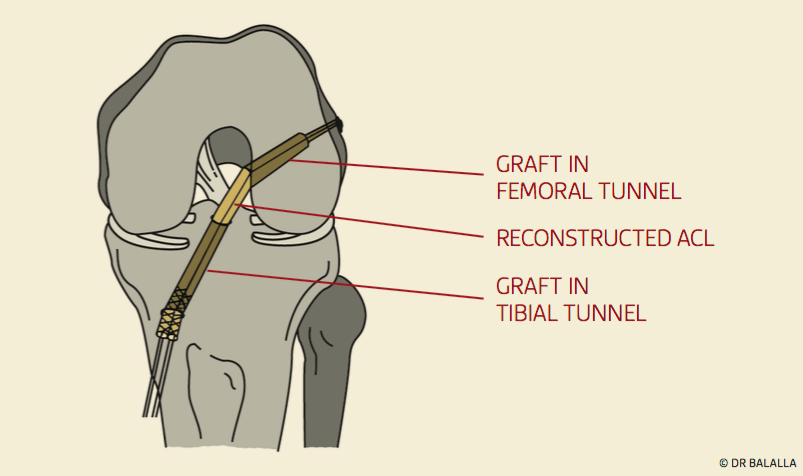
Reconstruction of the ACL using a tendon graft
Watch an animation of an ACL reconstruction
Arthroscopic video of a remnant-preserving ACL reconstruction