
Knee Arthritis and Knee Replacement
What is arthritis?
Knee arthritis is very common in patients 50 years and older. Arthritis is a condition which causes a degradation of the cartilage lining a joint, leading to a painful joint. Symptoms may include joint pain, tenderness, stiffness, locking (where the knee is unable to fully straighten), and sometimes an effusion (fluid in the joint). The knee typically is less painful at rest, and painful with prolonged activity. The knee may occasionally give way. In more severe cases, night pain may impair sleep.
There are many different reasons for arthritis, but the main type requiring operation is osteoarthritis. This can be separated into primary and secondary osteoarthritis. Osteoarthritis manifests itself as breakdown of the shiny smooth cartilage which lines the ends of the bone within the joint. These changes then affect the underlying bone. Cartilage damage is irreversible.
Primary osteoarthritis is related to the aging process and typically occurs in older individuals. Its cause is complex, with a genetic basis, occurring in previously intact joints and having no apparent initiating factor.
Secondary osteoarthritis can be the end result of many conditions which can affect a joint. Inflammatory conditions such as rheumatoid arthritis, or trauma to a joint, or any factor which changes the mechanical or metabolic environment of a joint, can lead to secondary osteoarthritis.
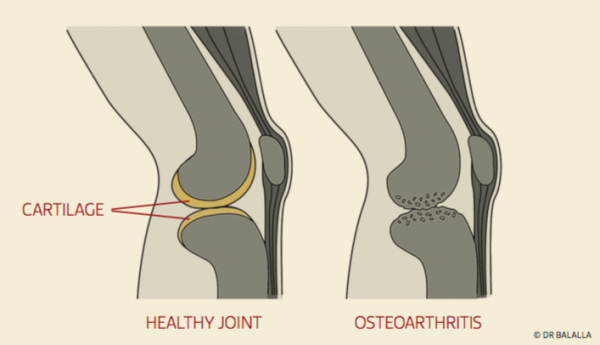
Diagram of normal and arthritic knees
Several factors may increase the risk of developing knee arthritis.
- Inherited risk
- Being overweight
- Ageing
- Female gender
- Trauma to the cartilage of the knee
- Knee instability and absence of a meniscus
- Heavy occupational loads
- High impact sports
- Acute or chronic inflammation of the knee
Knee arthritis can be diagnosed on standard x-ray films. Films performed while the patient is weight bearing are the most accurate for seeing the loss of space between the bones which indicates cartilage loss. For early arthritis, an MRI may be helpful.
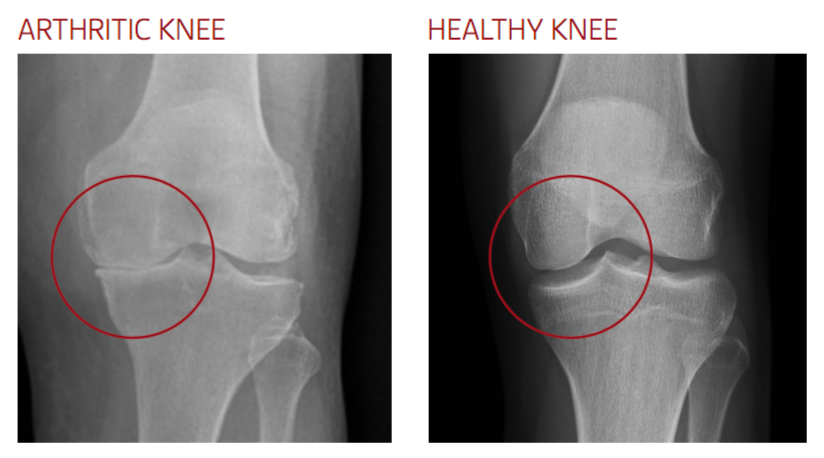
X-ray of normal and arthritic knees
How is arthritis treated?
Non Surgical Measures
Activity Modification
The initial treatment of osteoarthritis involves trying to modify activity to avoid pain and further damage. Impact exercises such as running should be avoided. Activities such as swimming or cycling are encouraged to keep active and maintain fitness.
Weight Loss
Weight loss can have a significant effect on the pain of arthritis. It has been demonstrated in studies that loss of 1 kilogram of bodyweight leads to a reduction of around 4 kilograms pressure within the knee joint when walking. This means that the pain of arthritis can be improved with weight loss as it will decrease the stress through the joint. Weight loss has an important role in the prevention of arthritis, with many studies noting the association of obesity and arthritis. One particular study showed a reduction of greater than 50% in the risk for arthritis with each loss of 5kg in a female of average height.
Dietary Supplements
The evidence for dietary supplements such as glucosamine or chondroitin is conflicted, with some studies showing a reduction of pain, but others showing no benefit. It does not help to regenerate cartilage.
Pain Medications
Simple pain medications may help to allow activity to continue, and are frequently used.
Injections
Corticosteroid injections may yield temporary relief for several months, but their effect is somewhat unpredictable. Repeated injections increase the risk of infection, or of abnormal crystal deposition within the joint known as chondrocalcinosis.
Viscosupplementation with agents such as hyaluronic acid may also yield relief for up to 6 months. As with corticosteroids, the effect of viscosupplementation is unpredictable, and repeated injections may be required. There is a risk with these injections of local inflammation, knee joint infection, and allergy.
Bracing
An unloading brace may be of use in patients who have arthritis confined to just the inside (medial) part of their knee. The brace shifts some of the load of weight bearing to the other side of the knee, reducing pain.
Arthritic patients may also benefit from simple knee sleeves, which can be purchased from pharmacies. These help with swelling control, and can help to modify the sensation of pain.
Surgical options for the arthritic knee
Ultimately, if pain persists despite medications, and is preventing you from performing your work, leisure, and family activities, surgery may be necessary.
The surgical options include:
Total Knee Replacement (TKR)
Total knee replacement involves removal of the diseased cartilage throughout the entire knee, and implantation of a metal and plastic prosthesis. Total knee replacement is most appropriate where the arthritis affects the majority of the knee, if there is significant deformity, or if there is an inflammatory basis to the arthritis, such as rheumatoid arthritis.
Unicompartmental Knee Replacement (UKR)
Unicompartmental knee replacement is appropriate where the arthritis is confined to one compartment of the knee. There are three main compartments of the knee – the medial (inner) compartment, the outer (lateral) compartment, and the kneecap (patellofemoral) compartment. Each of these may be selectively replaced, leaving the other compartments untouched. The advantages of unicompartmental knee replacement are of a smaller incision, less bleeding, less post-operative pain, reduced stay in hospital, and a feeling of a more “normal” knee.
Knee Osteotomy
Osteotomy is an alternative to knee replacement. The aim of knee osteotomy is to change the weight distribution of the knee to from an area of arthritis to an area which is unaffected. This is achieved by either cutting the bone above or below the joint, and fixing it with a plate and screws at a different, pre-determined angle. To achieve a good result, there must be an area of good cartilage to shift the load to, and the meniscus of that compartment must be intact. This operation is most suitable for patients who are young and wish to perform strenuous activity, such as manual labourers. Patients are unable to fully weight bear for 6 weeks until the osteotomy heals.
The treatment of your arthritic knee depends on the pattern of arthritis present within your knee, your age, and your activity requirements. This can only be determined after a careful assessment and discussion of the pros and cons of each type of surgery.
Please call my office to make an appointment if you would like to further discuss knee replacement options.
TOTAL KNEE REPLACEMENT
WHAT IS A TOTAL KNEE REPLACEMENT?
A total knee replacement is also known as a total knee arthroplasty or TKR. It is an operation that is performed for severe arthritis. Although there are variations in the design and philosophy of total knee replacements, there are also common features. All total knee replacements remove the failed cartilage within the knee joint from the femur and tibia, and replace them with a new metal surface on the femur, and a high-density polyethylene bearing on the tibia. The polyethylene bearing is most commonly held within a metal tibial tray that is bonded to the tibial bone. Frequently, the back surface of the kneecap is also replaced.

A total knee replacement fixed with bone cement.
WHAT IS MADE FROM?
The part which attaches to the thighbone, the femoral component, is most commonly made from cobalt-chrome alloy. It is a very hard and scratch resistant metal. Occasionally I also use a femoral component made of oxidised zirconium. This is thought to be even more scratch resistant, and avoids the possibility of allergy in patients who are sensitive to nickel.
The part which attaches to the tibia, or tibial component, is most usually made of titanium or stainless steel. To this is attached a bearing made of cross-linked high density polyethylene. It is against this surface that the femoral component moves.

WHEN SHOULD SOMEONE HAVE A KNEE REPLACEMENT?
A knee replacement should be seen a pain relieving measure which should be undertaken after all non-operative measure have been tried and exhausted. Patients who have severe pain, limited walking distance, night pain, or those losing significant quality of life due to knee arthritis, despite pain medications, may be suitable for total knee replacement.
WHAT ARE THE ALTERNATIVES TO TOTAL KNEE REPLACEMENT?
Joint replacements are likely to last longer when implanted in an older patient. Waiting several years to an age where activity is reduced may lead to less wear on the prosthesis. If possible, it is ideal to manage the symptoms with pain medications or joint injections until the pain is severe. Patients who are overweight may benefit from weight loss, which reduces stress within an arthritic joint. Only when the pain is not able to be controlled via these means should a knee replacement be considered.
In patients younger than 50, tibial or femoral osteotomy may be preferred to knee replacement. This involves cutting the bone of the tibia or femur, and re-aligning it so that the stress passes through the more normal areas of the knee rather than the arthritic areas.
If the arthritis only affects a small area of the knee, partial knee replacement (also known as unicompartmental knee replacement, or half knee replacement) may be an excellent alternative.
HOW IS A KNEE REPLACEMENT PERFORMED?
Knee replacement is performed under an anaesthetic. This may be a spinal anaesthetic, a general anaesthetic, or a combination of both. An inflatable cuff called a tourniquet is placed on the upper thigh to minimize bleeding during the operation. An incision is made running along the front of the knee. The knee joint itself is opened just on the inside of the kneecap. Using guides, the diseased cartilage is removed, and the bone ends shaped to fit the prosthesis. The ACL is always removed. Depending on the surgical plan, the posterior cruciate ligament may be removed. Trial components are inserted, and the knee is assessed. The soft tissues of the knee are then balanced so that even tension is observed, and the kneecap is tracking well. Once the trial is satisfactory, the definitive implants are bonded to the bone with a plastic grout called bone cement. Alternatively, some implants are have a special coating which the bone grows into – these implants are usually used in younger patients with good bone density. The knee is injected with a cocktail of medications designed to reduce pain and inflammation, and reduce bleeding. The layers of the wound are then closed.
WHAT IS PATIENT-MATCHED TECHNOLOGY?
I routinely use a relatively new technology called PSI, or patient-specific instrumentation. This involves imaging the knee with an MRI scan and long-leg x-ray films. A 3D computer model of the knee is then built. I then optimally position the implants to fit that specific knee. Once the plan is finalized, intra-operative guides which precisely fit that knee are 3D printed and sterilized. These guides are used instead of traditional long rods that are inserted into the canals of the tibia and femur to align the prosthesis.

Custom cutting guides for total knee replacement fitted to a bone model.
WHAT IS THE RECOVERY TIME FROM A TOTAL KNEE REPLACEMENT?
With newer techniques in soft tissue management and pain control, patients are returning to function faster. Patients can expect to spend 3-4 days in hospital following surgery, with the option of rehabilitation faster. I strongly encourage walking (with support) on the day of surgery, and early bending of the knee. Most patients are capable of driving within 2 weeks of surgery once their pain has settled, and they are off sedating medications. The exception to this is operating the clutch of a manual car, which may take a little longer. Office workers can consider returning to work after 3-6 weeks. Patients involved in more strenuous work, or prolonged standing, may take slightly longer. The knee gradually improves for up to 1 year after surgery.
AM I TOO OLD OR TOO YOUNG FOR A KNEE REPLACEMENT?
It is known that joint replacements do not last as long in younger patients than in older patients. Data from the Australian National Joint Replacement Registry shows that in patients under 55 years old having a total knee replacement 13.6% will have been revised, compared with 3.1% in patients over 75 years of age. Therefore in younger patients knee replacement is possible, but has a higher risk of wearing out due to their higher activity levels and demands.
In older patients, the main risk not that of the knee replacement having problems, but of the patient’s health being sufficiently robust for an anaesthetic, the operation, and the recovery period. There is no age limit to total knee replacement so long as the patient has well functioning heart and lungs and is of good general health and fitness.
In general, I advise patients who are in significant pain which reduces their quality of life, walking distance, and disrupts their sleep, and have exhausted non-surgical measures that they should consider total knee replacement. It is then a case of weighing up risks and benefits.
I HAVE ARTHRITIS IN BOTH KNEES. CAN THEY BE OPERATED ON AT THE SAME TIME?
Yes, depending on your general medical status, and heart and lung function. Performing both knee replacements in the one sitting has many advantages. These include shorter net hospitalization time, shorter rehabilitation time, and lower cost. However, due to the increased magnitude of the operation, there are higher risks. These risks have been shown to be only slightly higher, but of course are of concern. I limit my selection of patients for this procedure to those with adequate cardiac and lung function, and good general fitness. I would routinely require you to see your cardiologist or a general physician prior to surgery, and also to be transferred to the High Dependency Unit or to Intensive Care routinely after surgery. We also try to minimize the risk by using techniques during surgery to reduce bleeding, and to limit the amount of tissue affected by the surgery. These include spinal anaesthesia, a tourniquet, MRI based patient specific instrumentation, adrenaline infiltration of the tissues, and a clot-stabilising agent.
HOW LONG DOES A KNEE REPLACEMENT LAST?
The longevity of knee replacements depends on several factors:
- The design and materials used
- The way the patient uses their knee
- The positioning of the implant by the surgeon
Our understanding of prosthetic materials has improved with time, as has the quality of materials. We expect the current generation of implants to last at least 25-30 years.
Of course, knee replacements are less likely to wear or loosen in more sedentary patients than in very active patients. Patients engaging in running or impact sports may expect the implants to last less time.
Positioning of the implants by the surgeon is critical in ensuring the longevity of the knee replacement. Poorly aligned implants have been shown in studies fail at a higher rate. Higher failure rates have been noted in knees just 3° outside of ideal alignment.
The AOA National Joint Registry, which has been tracking all knee replacements for over 15 years, shows that the average survival of the prosthesis at 10 years is 94.5%.
CAN THEY BE RE-DONE WHEN THEY WEAR OUT?
Yes. However, re-operation is more difficult, and associated with a higher rate of complications. In the failing knee replacement, the risks of surgery need to be weighed up with the expected gains of re-operation. This is individual to each patient, and requires careful assessment by the surgeon. It is imperative that all the reasons for failure be identified and addressed, otherwise a suboptimal outcome may eventuate. Ensure that the surgeon performing the revision is well trained specifically in knee revision surgery, and has experience performing this surgery.
DO KNEE REPLACEMENTS HAVE METAL-ON-METAL ISSUES?
No. Although there have been several knee replacement designs which have failed and have been withdrawn, there have been no metal-on-metal bearing designs in use. Patients may rarely develop metal debris within a knee when the polyethylene wears or cracks completely, allowing the femoral component to directly rub on the tibial tray without the intervening polyethylene to protect it. These knees have to be revised, but have not had the catastrophic pseudo tumours or ALVAL related to metal-on-metal hip replacements.
WHAT ARE THE RISKS OF TOTAL KNEE REPLACEMENT?
The risks of knee replacement include (but are not limited to):
- Infection – rare but potentially catastrophic. Infection may need further operations to wash out or revise the implants. Very rare cases where the infection cannot be cleared despite removing the implants can end up requiring knee fusion or even amputation.
- Bleeding – this is becoming less of a problem with modern techniques, but around 5% of patients may need blood transfusion.
- Stiffness – persistent stiffness is less common with good implant positioning, but can occur. Most knees achieve slightly more bend than prior to surgery, but in rare cases the knee is left more stiff. Persistent stiffness should be investigated carefully as there may be an underlying reason.
- Pain – knee replacement is very effective at treating pain, but occasionally patients are left with pain after the surgery as settled. The cause for this needs to be investigated carefully as there is often an underlying cause. If no cause is found, there may be residual pain.
- Wear – the polyethylene in the knee can wear with time, requiring surgery. Sometimes a new polyethylene can be inserted, but occasionally the wear is associated with loosening of the metal components. In this situation, the knee replacement will have to be revised.
- Loosening – the bond between the metal and the bone can fail, leading to loosening and pain. This requires revision surgery.
- Dislocation or instability – the components of the knee replacement may jump or slide abnormally, leading to giving way of the joint. This may require revision of the knee replacement to a design with more intrinsic stability.
- DVT/PE – Deep Vein Thrombosis (DVT) involves formation of blood clot in the deep calf veins. This may occur after surgery, trauma, or even spontaneously. Knee replacement is associated with a higher risk of DVT. Special precautions are usually taken, including compression socks, pneumatic pumps, and either blood thinning tablets or injections. Even despite these measures, DVT can occur. DVT by itself causes calf pain and swelling, but its most concerning consequence is when the clot breaks free and travels to the lungs (called Pulmonary Embolism or PE), causing shortness of breath or chest pain. Very occasionally this can be serious or even life-threatening.
- Fracture – a very rare complication. If this occurs, further surgery or splinting may be required.
- Injury to nearby nerves and blood vessels – very rare, but may be associated with impaired log term function.
- Anaesthetic problems – Anaesthetic agents have been associated with allergic and anaphylactic reactions. In addition, the medications can depress the function of the heart and lungs. In older or more prone patients this may lead to heart attack, stroke, or cardiac failure.
How 3D-printed cutting guides are made
In the video below, my Fellowship mentor Mr Andrew Porteous performs a total knee replacement using patient-specific guides
UNICOMPARTMENTAL KNEE REPLACEMENT
WHAT IS UNICOMPARTMENTAL KNEE REPLACEMENT?
Uncompartmental knee replacement (UKR), also known as partial knee replacement or half knee replacement is an excellent option in patients where joint damage is confined to one section of the knee. There are 3 main “compartments” of the knee, the medial compartment, the lateral compartment, and the patellofemoral compartment.
Uncompartmental knee replacement involves replacing the surfaces of both the tibia and femur (in the case of medial or lateral UKR), or femur and patella (in the case of patellofemoral joint replacement). The remainder of the knee is left alone, except for the removal of any osteophytes, which are bone growths resulting from arthritis. Importantly, the cruciate ligaments, which are sacrificed in total knee replacement, are kept. This helps maintain normal joint motion and joint position sense.
Unicompartmental knee replacement:

Total knee replacement:

WHY HAVE A UKR INSTEAD OF A TOTAL KNEE REPLACEMENT?
UKR has many benefits over total knee replacement. The operation is smaller that having a total knee replacement, and as such is associated with
- reduced pain after surgery
- reduced blood loss
- better movement
- earlier return to function
Patients report a much more “normal” feeling knee, as more of the knee is preserved, and the knee rotates in a more normal motion. Studies on UKR have shown a greater proportion of highly satisfied patients when compared to total knee replacement, and fewer dissatisfied patients. Patients report a higher level of activity, and an increased ability to perform more difficult and strenuous activities.
UKR targets only the failing areas of a joint and is a more individualized treatment for a patient’s knee arthritis. Total knee replacement, although very successful, is a one-size-fits-all solution.
WHO IS SUITABLE FOR UNICOMPARTMENTAL KNEE REPLACEMENT?
Not everyone is suitable for UKR. It is very important to perform a thorough assessment prior to proceeding with surgery, involving a careful history of the pain and symptoms, physical examination, x-rays, and perhaps an MRI scan.
UKR is suitable for your knee if
- the pain is confined only to that segment of the knee
- the other compartments of the knee are normal on imaging
- you have a stable knee with no significant ligament problems
- you have good movement in the knee
- you do not suffer from an inflammatory joint condition such as rheumatoid arthritis
UKR may be seen as a single-step solution to patients with isolated single compartment arthritis. Typically, these patients are older, and lower in their activity levels. Alternatively, it can be used in younger patients as a smaller intervention allowing better function and earlier return to activity. This might be considered to be a staged intervention where years later a total knee replacement may need to be performed if the UKR were to wear out. Young patients who have this option can potentially enjoy the benefits of UKR while they are more active, and have a total knee replacement later in life when activity levels tend to be less.
CAN COMPUTER GUIDED SURGERY BE USED IN UKR?
WHAT ARE THE PROBLEMS WITH UKR?
Rates of UKR have fallen in Australia due to a perception that they are not as successful as Total Knee Replacement. The Australian National Joint Replacement Registry shows that there is a higher risk that a UKR will have to be re-done compared to a total knee replacement. After 10 years, 15.2% of UKR’s will have been re-done, compared with 5.5% of total knee replacements. The most common reasons for this are the implants loosening, or arthritis affecting the other areas of the knee.
Some of this difference in re-do rates may be because surgeons are more likely to revise a failing UKR than a failing total knee replacement because the surgery is more straightforward.
Regardless, it is important that UKR is done in a carefully selected patient, and by a surgeon with experience and a particular interest in UKR. Multiple studies have highlighted that surgeons with a higher rate of UKR have better overall results.
CAN I HAVE BOTH KNEES DONE AT THE SAME TIME?
Yes. Bilateral surgery is very well tolerated and is often the best way to proceed if the knees are equally affected. Of course, your general health would need to be taken into account to see whether the anaesthetic and surgery could be performed safely.
HOW LONG WILL I BE IN HOSPITAL?
Usually around 3-4 nights following surgery for single sided surgery, and 4-5 nights for bilateral surgery.
WHEN CAN I RETIRN TO WORK AND DRIVING?
I am happy for my patients to drive when their knee is bending well, and they are not in pain, and are off any sedating medications. Typically this is around 1-2 weeks following UKR surgery. Typically, office workers will return to work after 2-4 weeks and manual worker at around 4-6 weeks.
WHAT ARE THE RISKS OF UKR?
The risks of UKR include (but are not limited to):
- Infection – rare but potentially catastrophic. Infection may need further operations to wash out or revise the implants.
- Bleeding – this is minimal in UKR, and modern techniques cause minimal blood loss.
- Stiffness – stiffness can occur after scarring within the knee after surgery. Generally most patients have a similar range of movement to their pre-operative range.
- Pain – pain is expected after surgery, and usually settles within weeks. However some patients may have some mild ongoing pains.
- Wear – the polyethylene in the knee can wear with time, requiring surgery. Sometimes a new polyethylene can be inserted, but occasionally the wear is associated with loosening of the metal components. In this situation, the UKR will have to be revised.
- Loosening – the bond between the metal and the bone can fail, leading to loosening and pain. This requires revision surgery.
- Adjacent compartment arthritis – arthritis may begin to affect the other areas of the knee not replaced by UKR surgery. If this occurs, that area may either be suitable for another UKR, or the entire knee revised to a total knee replacement.
- Dislocation or instability – the components of the knee replacement may jump or slide abnormally, leading to giving way of the joint. This may require revision to a total knee replacement.
- DVT/PE – Deep Vein Thrombosis (DVT) involves formation of blood clot in the deep calf veins. This may occur after surgery, trauma, or even spontaneously. Knee replacement is associated with a higher risk of DVT. Special precautions are usually taken, including compression socks, pneumatic pumps, and either blood thinning tablets or injections. Even despite these measures, DVT can occur. DVT by itself causes calf pain and swelling, but its most concerning consequence is when the clot breaks free and travels to the lungs (called Pulmonary Embolism or PE), causing shortness of breath or chest pain. Very occasionally this can be serious or even life-threatening.
- Fracture – a very rare complication. If this occurs, further surgery or splinting may be required.
- Injury to nearby nerves and blood vessels – very rare, but may be associated with impaired log term function.
- Anaesthetic problems – Anaesthetic agents have been associated with allergic and anaphylactic reactions. In addition, the medications can depress the function of the heart and lungs. In older or more prone patients this may lead to heart attack, stroke, or cardiac failure.
