Knee Arthritis and Knee Replacement
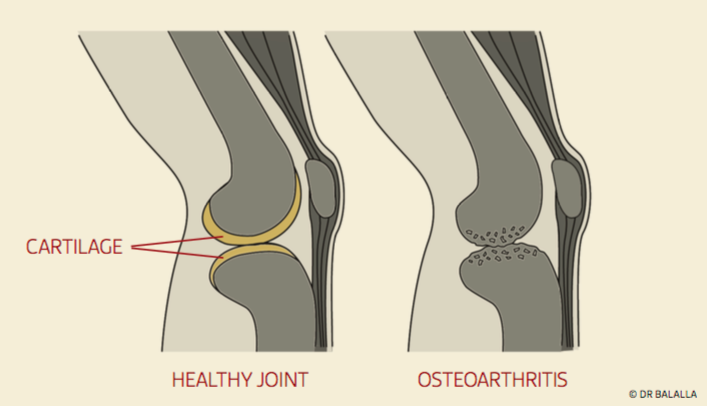
Arthritis is a condition which causes a degradation of the cartilage lining a joint, leading to a painful joint. Symptoms may include joint pain, tenderness, stiffness, locking (where the knee is unable to fully straighten), and sometimes an effusion (fluid in the joint). The knee typically is less painful at rest, and painful with prolonged activity. The knee may occasionally give way. In more severe cases, night pain may impair sleep.
There are many different reasons for arthritis, but the main type requiring operation is osteoarthritis. This can be separated into primary and secondary osteoarthritis.
Primary osteoarthritis is related to the aging process and typically occurs in older individuals. Its cause is complex, with a genetic basis, occurring in previously intact joints and having no apparent initiating factor.
Secondary osteoarthritis can be the end result of many conditions which can affect a joint. In ammatory conditions such as rheumatoid arthritis, or trauma to a joint, or any factor which changes the mechanical or metabolic environment of a joint, can lead to secondary osteoarthritis.
Osteoarthritis manifests itself as breakdown of the shiny smooth cartilage which lines the ends of the bone within the joint. These changes then affect the underlying bone. Cartilage damage is irreversible.
Several factors may increase the risk of developing osteoarthritis of the knee.
- Inherited risk
- Being overweight
- Aging
- Female gender
- Trauma to the cartilage of the knee
- Knee instability and absence of a meniscus
- Heavy occupational loads
- High impact sports
- Acute or chronic inflammation of the knee


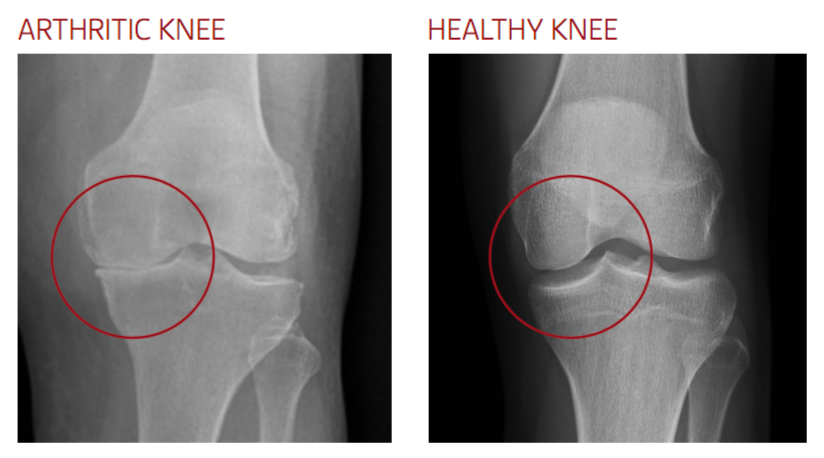
Arthritis can be diagnosed on standard x-ray films. Films performed while the patient is weight bearing are the most accurate for seeing the loss of space between the bones which indicates cartilage loss. For early arthritis, an MRI may be helpful.
Treatment options
The initial treatment of osteoarthritis involves trying to modify activity to avoid pain and further damage. Impact exercises such as running should be avoided. Activities such as swimming or cycling are encouraged to keep active and maintain tness.
Weight loss can have a signi cant effect on the pain of arthritis. It has been demonstrated in studies that loss of 1 kilogram of bodyweight leads to a reduction of around 4 kilograms pressure within the knee joint when walking. This means that the pain of arthritis can be improved with weight loss as it will decrease the stress through the joint. Weight loss has an important role in the prevention of arthritis, with many studies noting the association of obesity and arthritis. One particular study showed a reduction of greater than 50% in the risk for arthritis with each loss of 5kg in a female of average height.
With time, however, the pain may become more persistent and present during low level activity. Simple pain medications such as paracetamol , or non- steroidal anti-inflammatory drugs may help to allow activity to continue. The evidence for dietary supplements such as glucosamine or chondroitin is conflicted, with some studies showing a reduction of pain, but others showing no benefit. It does not help to regenerate cartilage.
Steroid injections may yield temporary relief for several months, but their effect is somewhat unpredictable. Repeated steroid injections increase the risk of infection, or of abnormal crystal deposition within the joint known as chondrocalcinosis.
Viscosupplementation with agents such as hyaluronic acid may also yield relief for up to 6 months. As with steroids, the effect of viscosupplementation is unpredictable, and repeated injections may be required. There is a risk with these injections of local inflammation, knee joint infection, and allergy.
An unloading brace may be of use in patients who have arthritis confined to just the inside (medial) part of their knee. The brace shifts some of the load of weight bearing to the other side of the knee, reducing pain. These braces can be very useful in younger patients who are unsuitable for joint replacement, and can also be used to predict a response to a knee osteotomy (see below).
Arthritic patients may also benefit from simple knee sleeves, which can be purchased from pharmacies. These help with swelling control, and can help to modify the sensation of pain.
Ultimately, if pain persists despite medications, and is preventing you from performing your work, leisure, and family activities, surgery may be necessary.
The surgical options include:
Total Knee Replacement (TKR)
This is most appropriate where the arthritis affects the majority of the knee, if there is significant deformity, or if there is an inflammatory basis to the arthritis, such as rheumatoid arthritis. It involves removal of the diseased cartilage throughout the entire knee, and replacement with a metal and plastic prosthesis. This prosthesis is ideally likely to last over 15-20 years.
Unicompartmental Knee Replacement (UKR)
The advantages of unicompartmental knee replacement are of a smaller incision, less bleeding, less post-operative pain, reduced stay in hospital, and a feeling of a more “normal” knee. It is appropriate where the arthritis is confined to one area of the knee. There are three main “compartments” of the knee – the medial (inner) compartment, the outer (lateral) compartment, and the kneecap (patellofemoral) compartment. Each of these may be selectively replaced. Arthritis may spread to other areas of the knee with time, and may require revision to a total knee replacement. The National Joint Registry shows that around 85% of UKR’s are functioning 10 years after implantation.
Knee Osteotomy
The aim of knee osteotomy is to change the weight distribution of the knee to from an area of arthritis to an area which is unaffected. This is achieved by either cutting the bone above or below the joint, and fixing it with a plate and screws at a different, pre-determined angle. To achieve a good result, there must be an area of good cartilage to shift the load to, and the meniscus of that compartment must be intact. This operation is most suitable for patients who are young and wish to perform strenuous activity, such as manual labourers. Patients are unable to fully weight bear for 6 weeks until the osteotomy heals.
The treatment of your arthritic knee depends on the pattern of arthritis present within your knee, your age, and your activity requirements. This can only be determined after a careful assessment and discussion of the pros and cons of each type of surgery.
Related blog posts
- When should I have a knee replacement?When is the right time to have a knee replacement? Many patients worry that a knee [...]Read more
- Kinematic Alignment of a Total Knee ReplacementKinematic Alignment is a customised method of positioning a knee replacement with the [...]Read more
- Uni knee is a good option to maintain functionI find that my patients who have had a unicompartmental knee replacement (UKR, [...]Read more

{kind=link}
{kind=link}