Kinematic Alignment is a customised method of positioning a knee replacement with the aim of restoring the native, pre-arthritic joint lines and rotational axes of a patients knee. While this may seem correct intuitively, this is not the way traditional total knee replacement is performed.
When performing a knee replacement, a surgeon chooses where to position each component on the bone. The surgeon must choose the depth of each cut, the angle each plane, and the rotation of each part. In engineering terms, there are six degrees of freedom. So when it comes to knee replacement, the most important question is: which is the correct position?
Malpositioning of a knee replacement can lead to pain, stiffness, or instability. The various technological choices available like conventional jigs, patient specific implant (PSI) planning and guides, computer navigation, and robotics are delivery methods. The surgeon ultimately plans the position of the implant, and the delivery method provides the means to replicate that plan.
Traditionally, knee replacements are aligned via a philosophy called Mechanical Alignment (MA). This aims to align every knee replacement the same way in all patients. The goal is a “straight” leg. This way of implanting a knee replacement was proposed in the 1980’s and was a response to the limitations of the designs and materials available at that time. It was thought that this means of positioning would improve the longevity of the implant via altering stress distribution, and didn’t take into account the individual anatomy of the patient. Most surgeons in Australia use mechanical alignment when performing a total knee replacement.
Mechanical alignment of a knee replacement seemed to improve the problems associated with less advanced materials and designs at the time, but over time, many of these shortcomings have been addressed. However, there is a lot of data regarding patient satisfaction with total knee replacement. Some studies suggest that up to 20% of patients are dissatisfied with their knee replacement. When we look at the natural alignment of native knees, we see that as with all biological phenomena there is a variation. Most knee are actually naturally not “straight”. In fact, only 2% of natural knees are straight when measured using the hip-knee-ankle (HKA) method on X-ray. Mechanical alignment seeks to put every patient into a “straight” alignment with a HKA of 0 degrees.
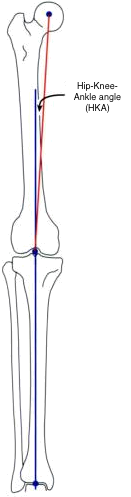
Measuring HKA
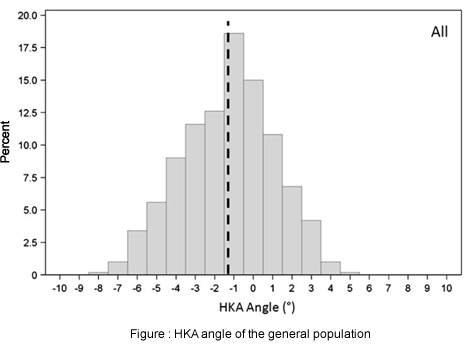
There is a large variation in natural knee alignment. Most patients don’t have a “straight” knee with an HKA of 0 (or 180 degrees depending on how it is measured)
The soft tissues of each knee are designed to rotate around the individual kinematic axes of that knee. In addition to their alignment, each patient has a specific, and different, set of rotational axes. Kinematic Alignment of a total knee replacement seeks to replicate these axes and the overall shape of the knee, and put the knee into the alignment it was in prior to the development of arthritis and deformity. Because the knee moves in a more natural way, my experience has been of better bending of the knee, and faster return to function. Patients report a more natural-feeling knee. In this technique, the position is customised to each and every knee.
To illustrate how different Kinematic Alignment can be compared with mechanically aligned total knee replacement, here is an example. In the X-ray below, the patient has arthritis present to an equal degree on both knees. The cut in yellow is typical of kinematic alignment, and closely follows the angle of the tibial joint line. The cut in red is mechanically aligned and is very different from the patient’s original joint angle.

This X-rays shows the difference between typical kinematic and mechanical alignment cuts in total knee replacement. Note the relationship of these cuts to the patient’s original joint lines.
Below is is an example of a kinematically aligned plan and a mechanically aligned plan on the same knee. This was performed using the 3D patient-specific planning software I use to align the knee replacement prior to surgery. The planned implant is visible as is the transparent 3D model of the patient’s bone. In the kinematically aligned knee the joint line matches the angle of the original joint line, where the mechanically aligned plan is very different.

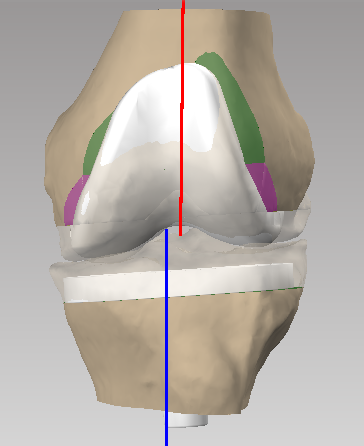
This image shows a mechanically aligned total knee replacement. The angle of the joint is very different from the angle of the tibial joint surface.
This image shows the planning for a kinematically aligned total knee replacement. Notice that the angle of the tibial implant matches the angle of the native joint.
Kinematic Alignment reproduces the flexion axis of the femur to align the femoral component. It has been known for over 100 years that the condyles of the knee have an equal radius of curvature. The centre of these circles describes the flexion-extension axis of the femur. The flexion extension axis can be calculated and replicated using 3D analysis.
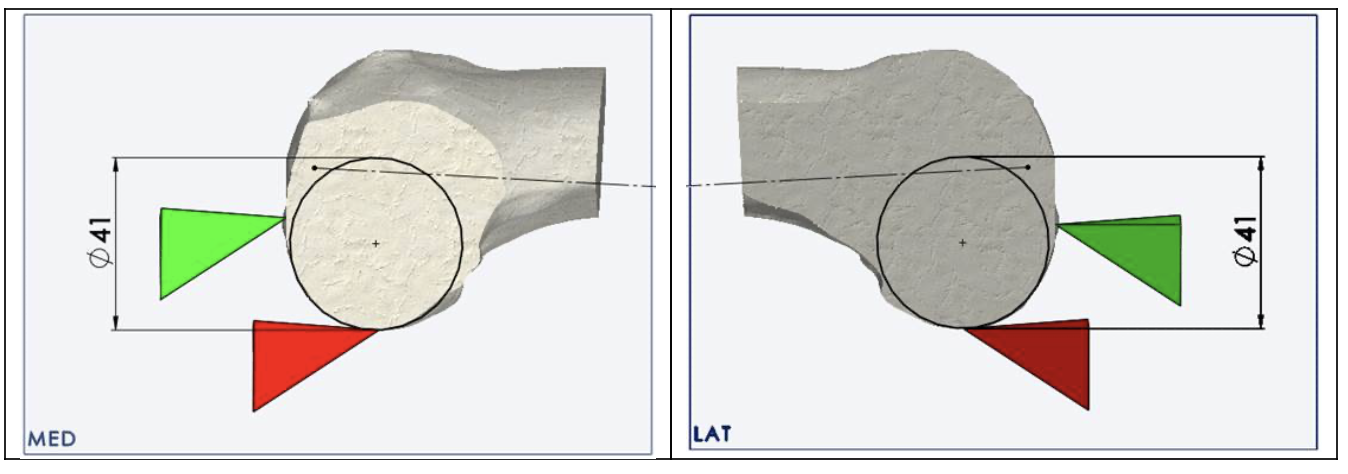
The flexion-extension of the knee can be calculated using analysis of a CT based model of each patient’s knee. This can then be replicated in kinematic total knee replacement.
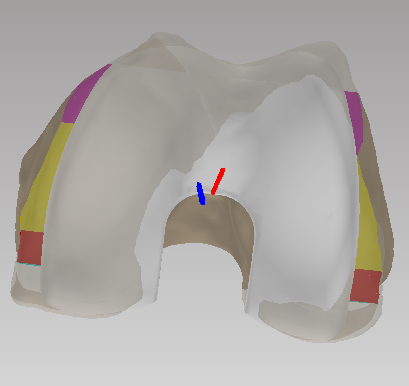
Kinematic placement of the femur replicates the femoral articulation
Kinematic knee replacement has shown excellent clinical outcomes, and many studies show it is as good or better than mechanically aligned total knee replacement. We have not seen an increased failure rate in kinematically aligned knee replacements compared with traditional mechanically aligned knee replacement.
I have performed over 300 kinematically aligned knee replacements, and I strongly believe that this is technique will give my patients the best outcomes following knee replacement.
If you would like to discuss kinematic knee replacement further, please call my office on 1300 695 633 or email enquiries@drbalalla.com.au
There are many articles available about kinematic knee replacement. Read more here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5103048