ACL ruptures in children and adolescents are relatively uncommon. The injury is usually related to sporting activity, and in fact many of these children play at a high level for their age. This age group accounts for only around 3% of ACL ruptures, but can present significant challenges in their treatment.
ACL ruptures in children have a poor prognosis without treatment or strict activity modification. Due to the specific challenges in reconstructing the ACL in these patients, many surgeons have advocated non-surgical management, or delaying treatment until the age of skeletal maturity, which is approximately 14 in girls, and 16 in boys. However, if these patients continue to be active in recreational play or competitive sports they risk cartilage or meniscal injury which can lead to early osteoarthritis.
Non-operative treatment of ACL injuries can lead to chronic instability and poor outcomes, with fewer athletes able to return to their sport at the same or higher level than in those undergoing reconstruction. In this study, observation of 23 patients who were treated non-surgically revealed that the natural history of the injury resulted in severe instability and poor function of the knee. Associated meniscal tears were present in 15 knees (65%). Three osteochondral fractures occurred (13%) and osteoarthritic changes developed in ten knees (43%) after 9 years.
Therefore, most orthopaedic specialists experienced in treating paediatric knee injuries would strongly recommend surgical reconstruction once the diagnosis of a torn ACL is made.
Treating these injuries presents increased challenges when compared with treating adults due to:
- Nearby growth plates
- Relatively small hamstring tendons for use as graft
- Difficulty restricting activity during the rehabilitation period
Avoiding the growth plates
The majority of growth in the leg occurs via the growth plates around the knee. These areas are made up of cartilage that grows out away from the joint. These growth plates can be injured by reconstructive surgery.
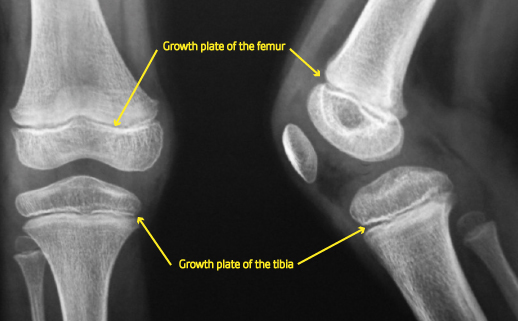
Usually, ACL reconstruction involves creating tunnels through these regions. This can injure the nearby area of the growth plate causing a bony bridge to form, connecting the two areas which normally separate with growth. This can cause asymmetrical growth across the plate, leading to deformity. Newer surgical techniques now allow the surgeon to avoid crossing the femoral growth plates entirely.
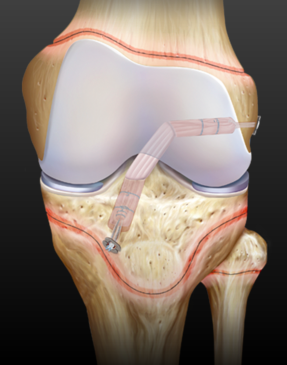
This technique allows the surgeon to completely avoid both growth plates
Graft choices
In children, hamstring tendons tend to be thinner than in adults. If these are harvested for graft, then the reconstructed ACL may be narrow and potentially weak. There are several options for addressing this problem. My preferred technique is to fold them each over four times instead of two, leading to a sufficiently thick graft. Quadriceps tendon may be used, but without taking any patella bone. Other options include using adult donor tendon, either as fresh tendon from a relative, or from a cadaver.
Patella tendon grafts are not suitable for harvesting from skeletally immature patients. Synthetic grafts are not used in these patients due to concerns about growth plate arrest and graft rupture and joint damage.
Rehabilitation
When the graft is being incorporated, it undergoes a period of weakness. During this time there is a risk of graft elongation or rupture. In adults it is easy to restrict activity after surgery, but in children this may be difficult due to their exuberant nature. Following ACl reconstruction in children ,they may require a period of bracing to limit activity and act as a reminder of their situation.