The anterior cruciate ligament is the most researched ligament in the entire human body. In 2015, over 1500 articles were published on the ACL alone, and the number keeps increasing each year.
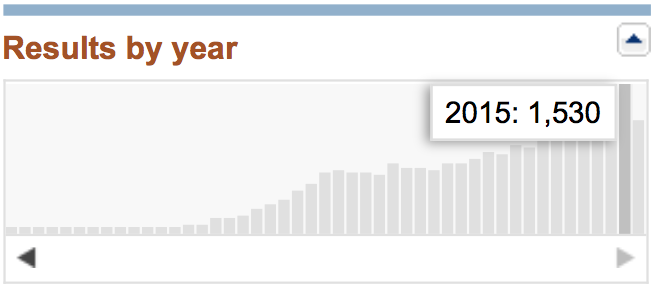
The number of scientific papers about the ACL has been steadily increasing.
With more knowledge, is logical that our techniques in treating ACL ruptures should be evolving, and hopefully providing our patients with better outcomes. So what are the new techniques surgeons are using?
ACL positioning
Our understanding of ACL anatomy continues to evolve and improve. The original concept of a cylindrical ligament was then replaced by a concept of two bundles. More recent studies suggest that there is a large variation in the shape of the attachment points of the ACL between patients, and that the active region of the ACL is in fact a band-like structure. Appreciating this individual variation can allow the surgeon to place the ACL reconstruction in the most appropriate position for that patient, rather than use a one-size-fits-all reconstruction. In my practice, I try to position the graft so that there are fibres in the footprint of each bundle.
-

- ajs.sagepub.com
-


- Freddie H. Fu. Orthopedics April 2011
Single hamstring grafts and short grafts
A recent study of 283 patients showed that graft diameters greater than 8mm have a much lower risk of failure than grafts smaller than 8 mm. We are now aiming for constructs of at least 8 mm.
Surgeons using hamstring grafts have traditionally harvest both the semitendinosus (semi-T) and the gracilis tendons. The semi-T is much thicker than the gracilis. In order to have sufficient length to allow fixation to bone, these two tendons were folded over on themselves, to form a four strand graft typically measuring 7-9 mm. By folding the thicker semi-T over itself 4 times, we can obtain a much bigger graft, typically measuring 8-10 mm. By using a single tendon, hamstring pain post surgery is significantly reduced compared to removing two tendons.
-


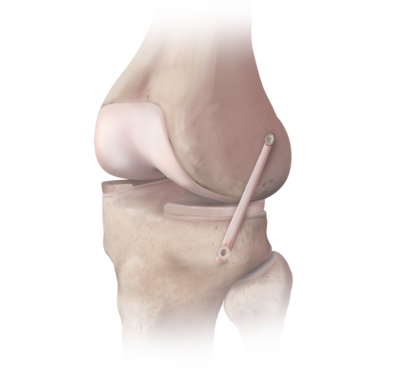
- Short 4-strand single hamstring graft
-

- Short graft ACL reconstruction
These single tendon grafts are much shorter than two-tendon grafts, and require alternative fixation devices. Although the graft is short, it is much stiffer due to its increased thickness, but also stretches less.
Remnant preservation
The torn stump of the ACL, or ACL remnant, is usually completely removed at the time of ACL reconstruction. This remnant contains blood vessels, collagen, and nerves. The remnant preservation technique involves keeping as much of the remnant as possible, and passing the graft through the centre of it, much like an arm through a sleeve. Studies on remnant preservation have demonstrated faster incorporation of the graft, stiffer stronger grafts, and better joint position sense.
Extra-articular ACL augmentation (ALL reconstruction)
It is thought that severe injuries of the ACL also injure the anterolateral ligament (ALL). The ALL is a fibrous band which runs with the capsule of the knee.
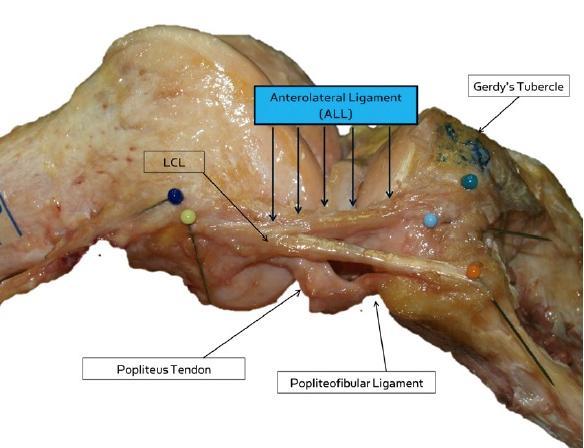
Dissection of the lateral (outer) side of the knee, showing the distinct band of the ALL
It may be that ACL reconstruction alone is insufficient to provide enough stability when the ALL is injured. The ACL sits near the centre of the knee, and resists rotation of the femur on the tibia. Sitting in the centre it has a small lever arm, and is in a relatively inefficient position.
In patients who have severe rotational laxity following ACL rupture, an extra-articular augmentation may be added to provide increased stability. Having a restraint to rotation on the outer edge of the knee has much more leverage in resisting rotation.
I offer ALL reconstruction to patients with severe rotational laxity, and in those whose previous reconstructions have failed. ALL reconstruction causes very little additional discomfort or stiffness, and does not require removal of any tendons.