Osteoarthritis (OA) of the knee is a common condition which causes pain. Typically the pain may come and go, and patients may experience periods of severe pain mixed with periods of little or no pain. As the arthritis progresses, the painful periods become more frequent and more severe. Once the pain is sufficiently severe, joint replacement may be necessary.
Generally I advise patients to consider knee replacement when:
- The pain affects sleep
- The pain affects work, recreational, and family activities
- Walking distance becomes very limited due to knee pain
Until this point, there are several options available to patients to help manage their pain.
Weight loss
Increased weight can lead to OA, and can worsen pain from OA. For a woman, a 5kg weight loss can reduce the risk of OA by over 50%.
Weight has a dramatic effect on pain from osteoarthritis. A 10kg weight loss can improve function by around 30%, as well as reducing pain. Weight loss is difficult, and needs a program of both exercise and dietary restriction. In younger patients I often recommend bariatric surgery (gastric sleeve surgery), which has been shown to improve knee pain and function.
Dietary Supplements
Glucosamine and chondroitin
Glucosamine is an amino sugar is used by the body to make glycosaminoglycans, one of the main components of the cartilage extracellular matrix. Results have been mixed, and its routine use is controversial. The amount of benefit may be very different between patients. The Osteoarthritis Research Society International (OARSI) recommends that “treatment with glucosamine and/or chondroitin sulphate may provide symptomatic benefit in patients with knee OA” and “if no response is apparent within 6 months treatment should be discontinued”. There is no evidence that glucosamine restores cartilage or protects it from damage. It acts purely as a pain reliever.
Fish Oil
Laboratory studies have shown that eicosapentaenoic acid and docosahexaenoic acid reduce proinflammatory mediators and increase joint lubrication in vitro. In addition, canine trials have shown clinically significant reductions in various symptom parameters. However, results of human clinical trials have not been consistently significant. There is no conclusive evidence for use, but some patients report reduced pain.
Medications
The most useful medications for the treatment of osteoarthritis include:
Paracetamol
This is widely available and effective, and generally very safe unless dosing exceeds the maximum amount of 4g/day. It can be used regularly for extended periods of time, although it is recommended that liver function should be checked if use is prolonged.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
NSAIDs are the most widely used pharmaceuticals in treating OA since many trials have confirmed their superiority to paracetamol for pain relief, but they also have a higher side effect profile.
This group of medications is related to aspirin, and includes ibuprofen, indomethacin, celecoxib, meloxicam, and many others. They work by reducing inflammation and therefore pain. They are very effective, but are not suitable for patients with kidney problems, or those who have a history of gastric or oesophageal ulcers. Newer generation versions such as celecoxib and meloxicam are generally considered to be safer due to less effect on the gut. Topical creams also work well, and have a reduced side effect profile.
Tramadol
Tramadol is a weak opioid which is commonly used in OA because it offers good pain relief with fewer adverse effects than other opioids. It is not addictive like other opioids and is suitable for longer term use.
Other opioids are generally not recommended for long term use due to their addictive nature and other side effects such as nausea and constipation.
Injections
Cortisone
Injected corticosteroids are a cost-effective non-invasive OA treatment. The rationale for their use is their anti-inflammatory effect through many complex actions, and the prolonged concentration of the corticosteroid in the joint fluid provides a high anti-inflammatory effect locally while minimizing the risk of side effects elsewhere in the body. Indeed, joint inflammation is common even in early OA and is linked to symptoms and structural progression of the disease. Steroids are very effective in controlling pain in mild-to-moderate OA, but less so in severe OA. The duration of effect can be around 3-6 months, but sometimes much shorter. Patients who respond with at least a 3 month benefit can have up to 3 injections per year. The effect tends to wear off with successive injections.
Hyaluronic Acid (Hylan)
Hyaluronic acid (HA) is a glycosaminoglycan that provides joint lubrication and shock absorbency and acts as the backbone for the proteoglycans of the extracellular matrix of cartilage. The initial theory behind using these injections was to restore missing levels of this molecule and reverse progression of the disease. Unfortunately this has not been shown to occur, but it has an anti-inflammatory effect, and is now used in clinical practice to reduce pain and improve function.
HA can be made as an extract from animal tissue, or as synthetic molecule. The products available differ in molecular weight, method of preparation, and dose, but clinical trials do not indicate a clear advantage of one product over another. The magnitude of the effect is similar to that of cortisone, but it lasts a little longer. It is generally more expensive than cortisone.
Platelet-rich Plasma (PRP)
Growth factors are stored in platelet α-granules, and have been shown to take part in the regulation of articular cartilage. PRP can be injected in high concentrations through platelet concentrates. There are a few available controlled studies which give overall support to PRP injections for knee OA treatment, which has a beneficial effect captured with placebo and slightly superior to that obtained with HA. There are better results in younger patients and those affected by early OA. PRP does not restore cartilage volume (thickness).

The preparation of platelet rich plasma. Non-surgical treatments for the management of early osteoarthritis. Filardo et al. Knee Surgery, Sports Traumatology, Arthroscopy
June 2016
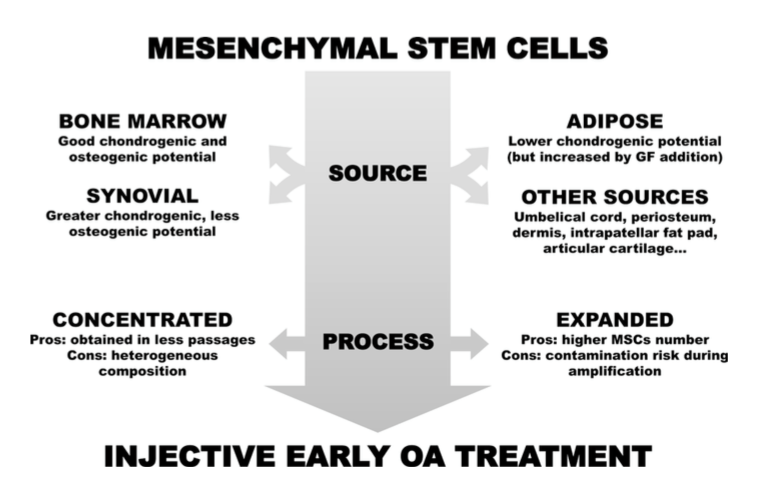
Stem Cells
Stem cells have also emerged as a treatment option to target OA by using their immunomodulatory and anti-inflammatory action, through direct cell–cell interaction or secretion of various factors. Cells may be harvested from adipose tissue (fat) or from bone marrow. The cells must be either concentrated or enhanced to yield the appropriate concentrations. There are many ways of preparing the cells but studies have shown the best results with bone marrow harvested cells which have been enhanced over a period of days prior to injection. Unfortunately this means an anaesthetic to harvest the cells from the pelvis, and then injection of the enhanced cells several days later. Stem cell injections are generally very expensive, and their effect not much better than the other injected treatments, and have a limit of duration of around a year. No studies have shown a restoration of lost cartilage volume, only a reduction in symptoms.
Exercise
Evidence shows that participating in an exercise program affected pain, physical function and quality of life in patients with knee osteoarthritis. The magnitude of this effect can be comparable to that obtained from anti-inflammatory medications. Positive results have been reported among all kinds of strengthening exercises as well as the different forms of aerobic activities (walking and jogging). In choosing an exercise, the best is to choose something that the patient enjoys so that they can continue it in the long term.
The pain of arthritis can flare at times. It is important to reduce exercise during these periods, rather than pushing through and worsening the pain. Exercise is important not only in maintaining fitness and reducing weight, but studies have also shown improved cartilage quality with activity.
Copyright Dr Bu Balalla 2016.